
HBGVs and BMDLs
Types of HBGVs
The "history" of HBGVs starts with the Acceptable Daily Intake (ADI). This concept was introduced in 1961 in Europe and was taken over by WHO/JECFA. Its unit is milligram or microgram per kg body weight of the consumer per day. So the unit demonstrates that it refers to the consumer, and not to the concentration in food or feed. The HBGV is derived for chemical substances or groups of substances that are intentionally added to food or feed, such as additives, pesticides and veterinary drugs (the so called residues). Sometimes it is called a "Provisional" ADI, to stress that it is based on very limited data and that it might be subject to an update in the near future.
A similar type of HBGV is the Reference Dose (RfD). The RfD is quite compliant to the ADI; it is derived using the same procedure, on the basis of the same data. It has the same unit as the ADI. This term is mostly used in North America (e.g. in the IRIS database of US-EPA).
Another well known HBGV is the Acute Reference Dose (ARfD). This guidance value is to be used in cases of acute exposure; most experts in exposure assessment use it for a single intake e.g. from one meal. It is mostly used in evaluations of pesticides. Its unit is milligram or microgram per kg body weight of the consumer. There is no unit for time here.
Another HBGV used in exposure assessment of chemicals in food or feed is the Tolerable Daily Intake (TDI). It is similar to the ADI but refers to contaminants and toxins whereas ADIs refer to residues. The term Tolerable is used here to express that we "tolerate" the contaminant rather than "accept" its presence, in contrast to residues. Besides of a Tolerable Daily Intake, one can also find the Tolerable Weekly Intake (TWI) or even a Tolerable Monthly Intake (TMI). Such HBGVs underline that the chronic exposure is more relevant than a short term intake. JECFA uses also the additonal term Provisional for most TDIs.
ADIs, TDIs, and RfDs are the HBGVs to be used in exposure assessments of chemicals in food or feed. Other types of values do also exist (e.g. AOEL, UL, AR, ..) but these do not point to maximal permissible exposure from food, but for the workplace, or refer to an optimal intake of nutrients.
Deriving a HBGV
The HBGVs are derived by scientific experts using appropriate data, e.g. scientific articles and reports of experimental studies. These studies can refer to studies with experimental animals such as mice and rats, but also with human volunteers or epidemiological studies. These experts usually join in scientific panels in international organizations such as JECFA and EFSA. Although more rare, it is also possible that HBGVs are derived only by national experts, or even by one expert, e.g. when the HBGV is urgently needed on a national level.
The experts take the available data, and start with selecting relevant data, eliminating others. Today, a systematic review is oft used for this. This process is based on expert opinion; there are no fixed rules or procedures how to weight the different data. Consequently there can be differences of opionion between the experts about the final result. This might lead to different HBGVs for the same chemical when derived by different panels (e.g. JECFA versus EFSA or US-EPA). After the selection of data, the experts define a dose that is considered the lowest effect dose in the studies. Here the type of observed effect, and the dose-response of that effect are most important.
Effect levels
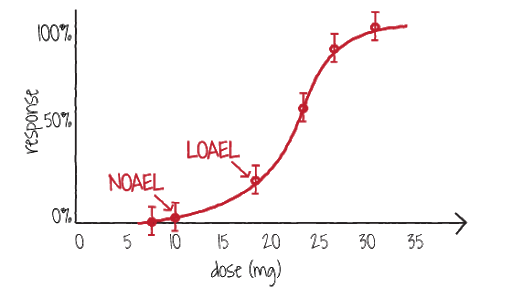 The most relevant dose level is the NOAEL. This acronym corresponds to the "No Observed Adverse Effect Level". It should be the highest level in the experimental study without effect (response). The effect should be reported as an adverse effect, i.e. injurious for animal or human. The effect should be Observed, meaning that it was actually seen in the study, e.g. a liver damage, or an increased or decreased level of an hormone or enzyme, or alike. One is now looking whether the various effect level are (statistically) different from the control level, or not. The control level is the level of the parameter of interest as measured in experimental animals or humans without exposure to the chemical. The terms used here are the "Lowest Observed Adverse Effect Level" (LOAEL), or "Marginal Observed Adverse Effect Level" (MOAEL). Sometimes these levels are reported without the term "Adverse" (e.g. NOEL for LOEL).
The most relevant dose level is the NOAEL. This acronym corresponds to the "No Observed Adverse Effect Level". It should be the highest level in the experimental study without effect (response). The effect should be reported as an adverse effect, i.e. injurious for animal or human. The effect should be Observed, meaning that it was actually seen in the study, e.g. a liver damage, or an increased or decreased level of an hormone or enzyme, or alike. One is now looking whether the various effect level are (statistically) different from the control level, or not. The control level is the level of the parameter of interest as measured in experimental animals or humans without exposure to the chemical. The terms used here are the "Lowest Observed Adverse Effect Level" (LOAEL), or "Marginal Observed Adverse Effect Level" (MOAEL). Sometimes these levels are reported without the term "Adverse" (e.g. NOEL for LOEL).
Setting the HBGV
The experts take an effect level, preferably the NOAEL. This is the basis for a HBGV like the ADI or TDI. The HBGV is now derived from the chosen effect level using safety factors (SF). These safety factors are actually extrapolation factors that take care of differences between the effect level and a "safe" exposure level for consumers. Most SFs are numbers of 10, and the common ADIs or TDIs are the NOAEL divided by 100 (i.e. 10 x 10). Additional safety factors of 10 can be used when selecting a LOAEL in stead of a NOAEL. Sometimes also SFs of 3 are being used, for example to extrapolate a MOAEL to a NOAEL. The SFs used to derive a HBGV are based on expert judgement of the panel members. There are guidelines for deriving SFs, but the underlying scientific basis for the weighing factors used as SFs is limited. Based on available data it can be concluded that such extrapolation factors of 3 and 10 are rather conservative. So the choise of SFs is a major point of discussion between experts for many HBGVs, leading to the observation that different panels come with different HBGVs although using the same scientific data ena effect dose.
Summary
Based on the approach of setting an ADI it can be concluded that HBGVs are derived from effect levels selected from experimental studies, lowered by various safety factors of 3 or 10. The factors are here to extrapolate from the experimental dose levels downto acceptable human exposure. Hereby it is assumed that the safety (resp. extrapolation) factors are sufficient in all cases to protect human health from adverse effects as seen in the experimetal studies.
Both the selection of the relevant effect and the SFs are based on expert judgement of toxicological experts; this can lead to different outcomes for different groups of experts. To overcome these differences, and using (informal) information of the European Commission, it can be concluded that EU Member States should use HBGVs as derived by EFSA, or from JECFA when an EFSA Opinion is missing.